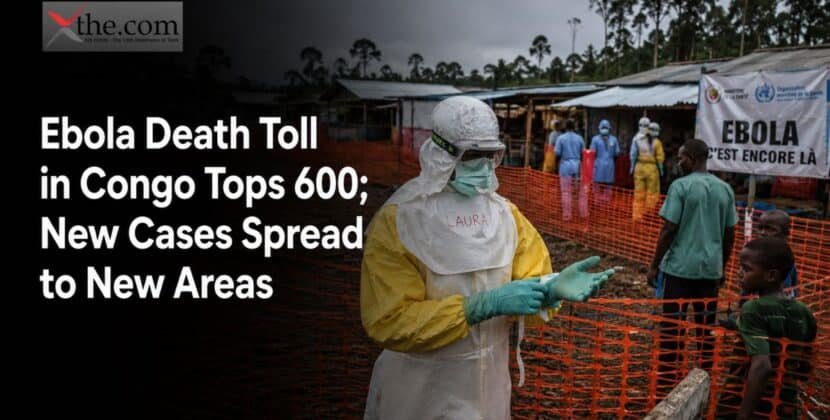








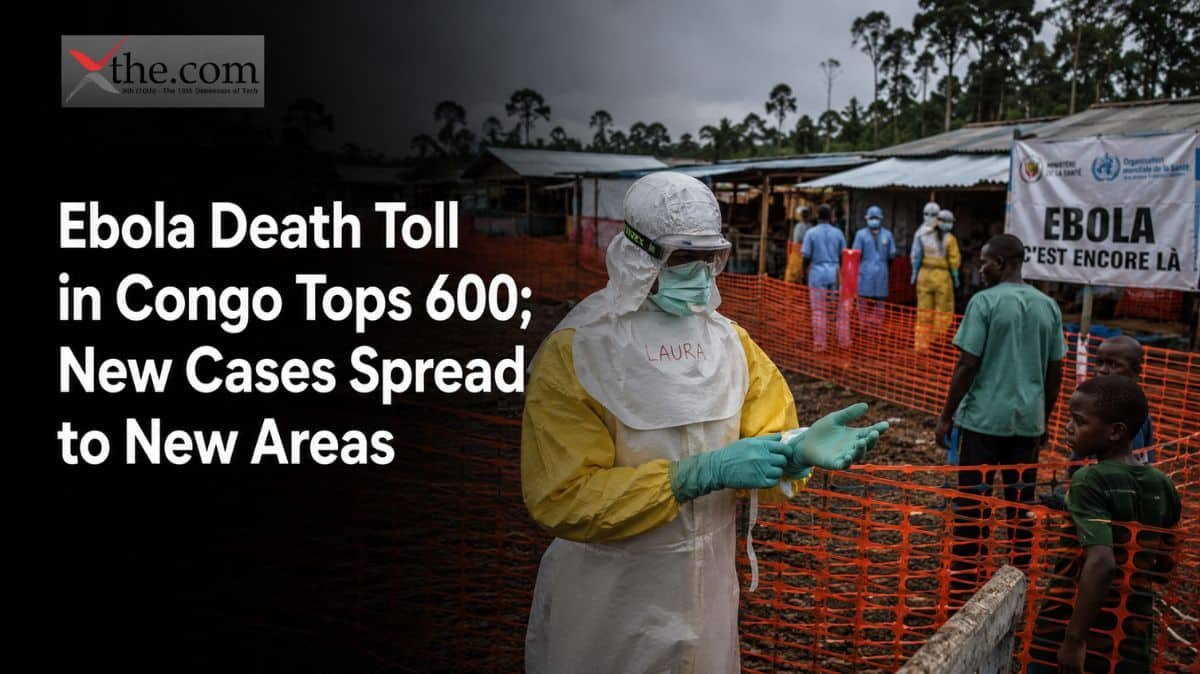
Kinshasa, DRC | Dateline: July 8–9, 2026
Six hundred people are dead, and the map of danger just grew larger. This is now a global health emergency Ebola 2026watchers cannot dismiss as a regional problem. The Ebola Congo death toll 600 milestone, confirmed by the Congolese health ministry this week, would be grim enough on its own. But the more alarming signal buried in the same government report is geographic: suspected infections have now surfaced in Tshopo and Haut-Uele, provinces that had recorded zero cases since the crisis began. The Ebola DRC 2026 outbreak has officially outrun its original containment zone, and the implications stretch from rural health posts in the Congo Basin to boardrooms at the world’s largest vaccine manufacturers.
A Fast-Moving Outbreak Enters New Territory
The Democratic Republic of Congo declared the outbreak on May 15, after the virus had already been circulating undetected for weeks in Ituri Province. By early July, confirmed cases nationwide had climbed past 1,750, and the Congo Ebola new provinces development — two suspected infections identified in Kisangani, the capital of Tshopo, marking the outbreak’s spread to a fourth province. One of these patients is linked to the Nia-Nia health zone in Ituri, but the other has no known connection. This worries epidemiologists even more than the rising death toll, as it points to community transmission that has not yet been tracked.
This crisis is moving quickly. The Africa Centers for Disease Control and Prevention says it is the fastest-growing Ebola outbreak ever seen in Africa. Thirty-seven out of 104 health zones in the DRC now have confirmed cases. North Kivu has reported 149 cases and 88 deaths. South Kivu, though less affected, has already lost one of its three confirmed patients. Each new affected province adds to the challenges facing a health system already under strain.
Why Bundibugyo Virus Changes the Calculus
What makes this outbreak different is the virus behind it. Unlike the Zaire ebolavirus that caused the 2014–2016 West Africa epidemic and other recent outbreaks for which licensed vaccines are available, this one is caused by the Bundibugyo virus. This rarer species was last seen in large numbers over ten years ago, and there is currently no licensed vaccine or approved treatment for it. In past Bundibugyo outbreaks, the fatality rate has ranged from 30% to 50%. This outbreak is also happening in an area already affected by armed conflict in eastern Congo, where attacks on health facilities and a lack of funding have made contact tracing very difficult.
Helping people in the newly affected areas is even harder. Tshopo and Haut-Uele are hundreds of kilometers from where the outbreak started. The roads frequently flood during the rainy season, and rivers are the only dependable way to travel. Vaccination campaigns and contact-tracing teams that took weeks to set up in Ituri now have to start over in places with little or no infrastructure.
The Global Health Emergency Ebola 2026 Response
The World Health Organization acted quickly. On May 17, the WHO Director-General declared the outbreak a Public Health Emergency of International Concern, the group’s highest alert level, after the Bundibugyo virus was found to have spread from the DRC to Uganda, where a Congolese man died in Kampala. This declaration triggered coordinated international funding and surveillance under the International Health Regulations, and it remains in force as the Congo Ebola 2026 WHO response effort scales with the outbreak’s geographic spread. The Africa CDC issued a parallel declaration, a Public Health Emergency of Continental Security, showing how seriously regional health officials view the cross-border threat.
Funding has followed the emergency, though not always evenly. The United Kingdom pledged up to £20 million for affected communities. The U.S. State Department later announced $112 million in aid for protective equipment, screening, and diagnostics. However, cuts at American health agencies have made the U.S. less visible on the ground than in past outbreaks, according to independent observers. The European Union added €15 million. Gavi, the Vaccine Alliance, has committed $50 million through its First Response Fund, with some money set aside to protect health workers and up to $40 million to accelerate the development of a vaccine that does not yet exist.
The Vaccine Gap Investors Need to Understand
This is where the market situation becomes more complex, and clear information is more important than hope. Merck’s Ervebo and similar vaccines for the Zaire species are in the Gavi-funded emergency stockpile, but they target a different virus. Now, manufacturers and researchers are working quickly to determine whether any current vaccine candidates can protect against the Bundibugyo virus. Clinical trials for an experimental treatment started last week at the Evangelical Medical Center in Bunia. About 2,000 doses of the Ebola vaccine are already in the DRC, ready for trials if WHO experts deem it justified, but no company has a licensed vaccine for this strain yet. Gavi and UNICEF have asked manufacturers to show interest in developing Bundibugyo-specific vaccines, with early research funding from the Coalition for Epidemic Preparedness Innovations. For pharmaceutical investors and global health funders, there is a real opportunity here, but it is still in the development stage, not ready for stockpiling.
Ebola DRC Spread Unaffected Areas: What Comes Next
Anyone who has followed Ebola outbreaks in the Congo Basin knows that containment in one zone buys time, not victory, if surveillance in neighboring provinces lags. The larger pattern of Ebola DRC spread unaffected areas reporting is precisely what worries the WHO’s Emergency Committee, because each new health zone means responders must rebuild logistics chains from the ground up. Ebola Congo 600 deaths new provinces affected will likely continue unless contact tracing in Tshopo and Haut-Uele improves quickly. Health officials in Kinshasa have called for more case detection, safe burials, and community involvement—steps that worked against Zaire ebolavirus outbreaks but are now being used against a virus with much less experience behind it.
The next month will show whether international funding turns into real action quickly enough to stop a virus that has already spread farther and faster than expected. “Ebola death toll Congo tops 600 July 2026 new cases suspected previously unaffected provinces” is this week’s headline. Whether this becomes the story of a contained crisis or a growing one now depends on choices made in provincial health offices, in Geneva, and in vaccine company boardrooms in the coming weeks. This makes the “Congo DRC Ebola outbreak 2026 600 deaths spread new areas WHO response investor healthcare impact” story one that global health funders and pharmaceutical leaders cannot afford to ignore.
Source: Ebola death toll in Congo tops 600. New cases also suspected in previously unaffected provinces